
Case 2 - 50 year old male with renal tumor
- Sep 26, 2020
- 3 min read








Scroll down to see final diagnosis and case discussionDiagnosis: Clear cell renal cell carcinoma
Pathologic findings:
Clinical features
· Most common type of renal epithelial tumors, about 70% of renal cell carcinomas.
· Commonly seen in adults (6th-7th decades) with M:F ratio 2:1
· Most common clinical sign is hematuria.
· Clinical triad: flank mass, pain, and hematuria.
· Conditions associated with RCC in some cases: von Hippel–Lindau (VHL) disease, Acquired cystic disease of the kidney, Adult form of polycystic kidney disease, Birt-Hogg-Dubé syndrome (germline folliculin mutation), Hereditary leiomyomatosis and RCC syndrome (germline fumarate hydratase mutation), Hereditary paraganglioma syndrome (germline succinate dehydrogenase mutation), Tuberous sclerosis, Neuroblastoma, PTEN Hamartoma Tumor Syndrome (germline PTEN mutation), Hereditary papillary RCC syndrome, Hemoglobinopathy (most commonly sickle cell trait), BAP1 tumor predisposition syndrome and MiTF-associated cancer syndrome
· Investigation of a suspected renal mass begins with CT scan or MRI.
Gross pathology
· Single well delineated renal cortical mass, 5% - multifocal.
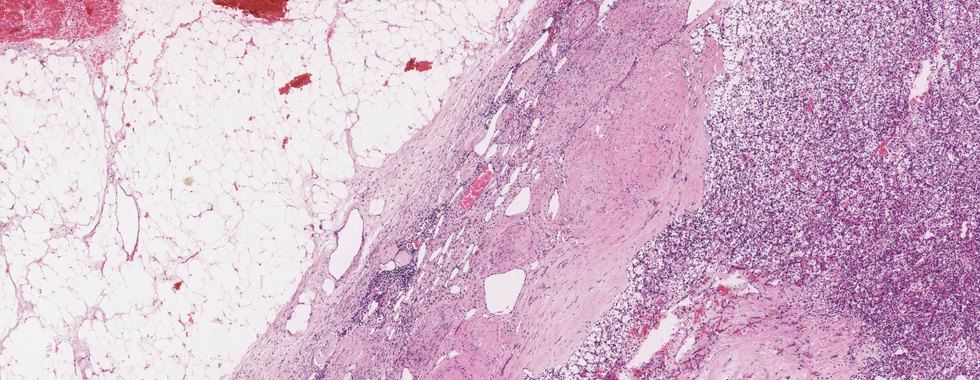
· Solid, golden-yellow tumor, sharply separated from the surrounding tissues by a fibrous pseudocapsule.
· Variegated appearance with presence of hemorrhage, necrosis, calcification, and cystic change.
· Submit sections to demonstrate the relationship of the tumour to kidney parenchyma, renal pelvis, major blood vessels, renal capsule, perinephric fat and adrenal gland if present.
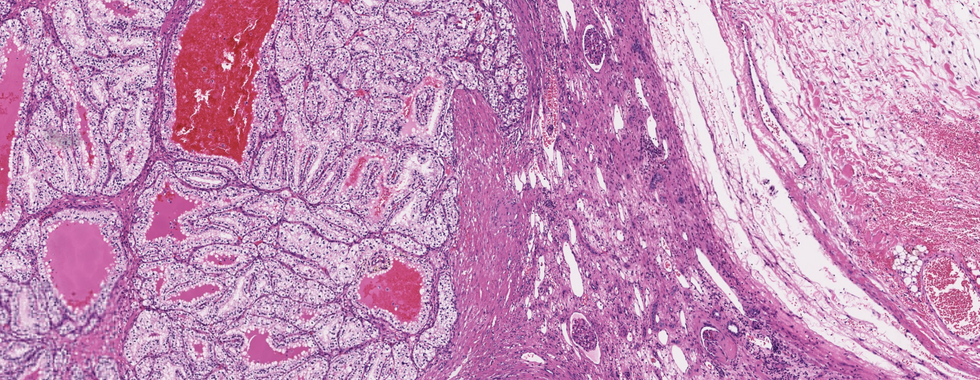
Microscopic Pathology
· Predominantly solid tumour pattern with alveolar and acinar tumour cell arrangement separated by a characteristicvascular stroma showing prominent network of small, thin-walled blood vessels.
· Other patterns noted, include trabecular, microcystic, and pseudopapillary, tubular in rare cases. Sarcomatoid differentiation with spindle cell formation can be seen.
· Individual tumor cells are large with optically clear to deeply granular cytoplasm.
Staging and grading
World Health Organization/International Society of Urological Pathology Grading System for clear cell renal cell carcinoma and papillary renal cell carcinoma
· Grade 1: Nucleoli are absent or inconspicuous and basophilic at ×400 magnification
· Grade 2: Nucleoli are conspicuous and eosinophilic at ×400 magnification and visible but not prominent at ×100 magnification
· Grade 3: Nucleoli are conspicuous and eosinophilic at ×100 magnification
· Grade 4: Extreme nuclear pleomorphism and/or rhabdoid differentiation and or sarcomatoid differentiation.
Special Stains and Immunohistochemistry
· Reactive: Cam 5.2, AE1/3, EMA, vimentin, CD10, CA9, and RCC antigen, PAX-2 and PAX-8
· Non reactive: Keratin 34BE12
· Rarely reactive: S100 or CEA
Molecular pathology
The majority of sporadic clear cell RCC shows chromosome 3p deletion The four most commonly mutated genes are VHL, PBRM1, BAP1, and SETD2 34% to 56% of sporadic cases show VHL gene mutation. and 20% show promoter methylation.
Prognosis
The overall 5-year survival rate is approximately 70%.
Differential diagnosis
Chromophobe renal Cell Carcinoma
· Nonencapsulated tumour mass with cut section showing homogenous and light brown appearance
· Cytoplasm is translucent and reticulated, not clear unlike clear cell RCC
· Positive Hale’s colloidal iron staining
· Diffuse positivity with cytokeratin 7
Papillary renal Cell Carcinoma
· Histiocytes with intracellular hemosiderin are commonly seen
· CK 7 and AMACR positive
· CA9 negative
· Trisomy 7 and 17 and loss of Y chromosome in male patients
Clear Cell (tubulo) papillary renal Cell Carcinoma
· Characteristic pattern of branched acini or ribbons lined by low-grade clear cells
· Nuclei polarized away from basement membrane toward the luminal surface of the acini and glands
· Cytokeratin 7, CA9, and keratin 34BE12: positive
· CD10 and AMACR: negative
Adrenocortical Carcinoma
· Cytoplasm is flocculated, not clear unlike clear cell RCC
· EMA and cytokeratin: negative
· Inhibin and calretinin: positive
Epithelioid angiomyolipoma
· Other components also noted, like fat or dysmorphic vessels
· Typical multinucleated epithelioid cells
· Positive for melanocytic markers, such as HMB-45, Melan A, tyrosinase but negative for epithelial markers
· MiTF positive
How to sign out the case
Left kidney, Radical nephrectomy specimen: Renal cell carcinoma, clear cell type.
WHO/ISUP Grading System: Grade 1, 2, 3 or 4
Sections from renal pelvis, vessels, capsule, perinephric fat and adrenal gland: Free or involved by tumour
Lymph nodes: Free or involved by tumour
References
Surgical Pathology Dissection: An Illustrated Guide 2nd edition, Chapter 33 William H. Westra, M.D., et al.
Rosai and Ackerman’s Surgical Pathology, 11th edition. Chapter 24, Jesse K. McKenney.
Mills, Stacey E. Sternberg’s Diagnostic Surgical Pathology. 2015, Chapter 42, Satish K tickoo, Victor E. Reuter
Differential diagnosis in surgical pathology, Third edition 2015, Chapter 10: Cristina Magi-Galluzi, Laura Barisoni, Ming Zhou.



Comments